
Back Pain and Balance: A New Way to Think About Back Rehab

Essential Points:
Back pain isn’t just structural, it’s neurological and movement-based. Pain changes how the nervous system controls movement, often leading to stiffness, altered muscle timing, and reduced body awareness, which can impact balance before strength even declines.
Balance and back pain likely reinforce each other in a cycle. Pain leads to cautious, less adaptable movement → poorer balance → inefficient movement patterns → increased stress on the spine → more pain.
Balance training may help by retraining the system, not just the spine. It improves coordination, restores movement variability, reduces fear, and reconnects the body as a whole, often making movement feel safer, more natural, and less painful.
Prefer to listen? Here’s a quick breakdown with a few extra insights:
When I was a relatively new physical therapist, about two years into practice, I treated a large number of patients with back pain. While I used strengthening, mobility work, and traditional rehabilitation approaches, my treatment style included something that stood out, a surprising amount of balance training.
Standing tasks, weight shifts, unstable surfaces, and movement challenges became regular parts of sessions, exercises that didn’t seem obviously related to the spine. Many of my earliest Science of Falling Instagram posts were based on these “balance games,” as I called them at the time. My clinic manager, an excellent clinician fond of rehab like the McKenzie Method, likely viewed the approach as unconventional, though he always allowed me the space to explore it.
And something interesting kept happening.
Patients improved. Pain decreased, confidence increased, and sessions became more engaging than the repetitive exercise routines many had experienced before. People didn’t just get stronger or more flexible, they moved more comfortably in their bodies.
At the time, I couldn’t fully explain why. Maybe balance training strengthened surrounding muscles with low-load movement. Maybe it encouraged movement variability or reduced fear of motion. Or maybe balance and back pain were connected more deeply than I realized.
Despite spending years thinking about balance through Science of Falling, I had never fully explored the research behind this observation, until now. Modern science suggests balance and back pain may be linked in ways that could reshape how we understand both. While not every connection is fully established, emerging research across pain science, motor control, and balance provides enough overlap to explore how these pieces may fit together.
So the question becomes:
Is balance training helping back pain accidentally, or is balance itself deeply connected to how the spine functions?
What is Balance?

When most people think about balance, they picture standing on one foot or trying not to fall over. But physiologically, balance is far more complex, and far more interesting.
Balance can be thought of as the central nervous system’s (your brain and spinal cord) ability to maintain orientation and stability in a constantly changing environment in conjunction with the joints and muscles.
To do this, the nervous system relies on three primary sources of information, what I often call the three bodily balance systems:
Vestibular system: Senses head motion, acceleration, and gravity through structures in the inner ear
Visual system: Provides environmental reference points and motion cues through vision
Somatosensory system (proprioception): Detects body position and movement through receptors in muscles, joints, connective tissue, and contact with surfaces
These systems work together continuously. The brain integrates their input and dynamically adjusts which signals it relies on most depending on the situation, a process known as sensory reweighting.
Balance Is Continuous Prediction and Correction
Standing upright is mechanically unstable. (1, 2) Even small changes from completely vertical create gravitational forces that would cause us to fall if the body didn’t respond immediately with reflex and muscular action.
Balance, therefore, is not static. It is a continuous loop of sensing, predicting, and correcting movement in real time.
In simple terms, and how I often explain it to patients, the brain is constantly deciding which muscles activate, in what order, and with how much force to keep the body upright against gravity. What we perceive as a “wobble” is not failure, but the nervous system actively solving a movement problem.
Balance Requires the Whole Body
Although balance corrections often appear to happen only at the feet or ankles, control involves the entire body. (3)
The trunk and spine play a particularly important role because they sit near the body’s center of mass (CoM). The CoM is essentially the body’s “balance spot” which we actively try to keep over our base of support (BoS) to remain upright. Small adjustments at the ankles can fine-tune whole-body position, while larger or faster disturbances recruit the trunk and hips to generate more aggressive corrective movements. (4) The majority of balance related movements are performed to keep your CoM over your feet.
Consequently, balance is not just a skill of the feet, it is a whole-body coordination process centered around the trunk, and more specifically the CoM. The spine is not simply being stabilized during balance, it can actively participate in the control system itself if needed.
And this brings us directly to back pain.
The Traditional View of Back Pain, And Its Limits

For decades, back pain has most commonly been explained using a structural model. Pain was thought to come primarily from identifiable physical problems such as:
disc degeneration or disc bulges
joint irritation
muscle tightness or weakness
visible abnormalities on X-ray or MRI.
While these physical deficiencies can sometimes matter, modern research has shown that the relationship between structure and pain is far less straightforward than once believed. (5) That may also be why the diagnosis of “non-specific low back pain” is so prevalent in healthcare today.
Imaging Findings Often Don’t Match Symptoms
In fact, structural findings on imaging frequently appear in people without any pain at all. (6) MRI studies consistently demonstrate that structural changes alone are unreliable indicators of a person’s pain experience, unless it lines up with the symptoms they are presenting with. Because of this, clinical guidelines recommend avoiding routine imaging for most cases of low back pain initially unless serious medical conditions are suspected, as imaging rarely improves outcomes when no red flags are present. (7)
Imaging can even have unintended psychological effects. Terms like degeneration, bulge, or wear and tear may create fear or catastrophic thinking, an example of the nocebo effect, where negative expectations amplify pain, disability, or anxiety. (8, 9) Research shows that how patients interpret imaging findings can meaningfully influence their pain experience even up to a year later.
This does not mean structures never matter. It means structure alone rarely explains the full picture.
Pain Is a Nervous System Experience
Modern pain science understands pain as an output of the nervous system, a protective response influenced by many factors, including:
sensory input
past experiences
expectations
movement behavior
perceived threat
Physical structural health plays a role, but pain is ultimately an interpretation of many signals, not just a direct measurement of tissue damage. (10) This explains why two people with similar imaging findings may have completely different pain experiences.
Let me give a simple personal example.
Over the course of my life I’ve suffered from many papercuts. Sometimes I am so focused and busy that I don’t even realize I’ve been cut. Minutes later I might notice a small amount of blood on my finger or work surface. After investigating I realize I cut myself and then all of a sudden start to feel the throb of pain in my finger.
But, pain wasn’t my first signal of the injury, rather it was the sight of blood. Pain only started after I realized I was injured. Consequently, the injury itself didn’t immediately register as painful, but once I became aware of it, my perception changed and the pain became noticeable.
Attention increased, protection increased, and the sensation of pain became apparent.
Rather than pain being switched on consciously, the nervous system continuously updates its assessment of threat using incoming sensory and contextual information. What we perceive, and when we perceive it, is shaped as much by interpretation as by tissue damage itself.
Pain Shapes Movement Behavior
Pain can lead to altered movement patterns. (11, 12) People naturally move more cautiously, becoming stiffer, slower, and less variable in movement. Over time, these protective strategies can unintentionally reinforce pain and reduce movement adaptability, while also shifting load to other areas of the body.
But this relationship doesn’t only go one direction. The way we move can also influence, at least in part, how pain is experienced.
A simplified way to summarize this idea is:
Act fine, feel more fine. Act injured, feel more injured.
This doesn’t mean ignoring pain or forcing movement, but rather that how we move can influence how safe the body feels.
Not because pain is imaginary, but because movement patterns continuously influence how the nervous system evaluates safety. You might still be injured, but allowing as much comfortable and tolerable movement as possible can lessen the perceived threat of the injury to your brain, while also reducing unnecessary stress on the body.
The Overlooked Question
So let’s take this a step further:
If pain changes how muscles activate…
If it alters posture and movement strategies…
If the nervous system becomes more protective…
What happens to balance?
And more importantly:
If movement control changes during pain, does balance change too?
That question is where the connection between back pain and balance truly begins.
What Research Shows: Back Pain Changes Balance

If balance depends on coordinated sensory input and precise muscle timing, what happens when pain enters the system?
Research over the past two decades shows that people with low back pain don’t just experience discomfort, they move differently, often before measurable strength loss appears.
Motor Control Changes
One of the most consistent findings in back pain research involves changes in how trunk muscles activate during movement. (11, 12, 13) Studies show individuals with low back pain commonly demonstrate:
Altered trunk muscle timing
Delayed anticipatory postural adjustments
Increased stiffness or muscular guarding
Reduced automatic movement responses
In healthy movement, deep trunk muscles often activate before limb motion begins, stabilizing the spine in anticipation of movement. (14) In people with back pain, this feed-forward activation is often delayed or less effectively coordinated. (15)
The nervous system shifts from an efficient predictive strategy to a more cautious reactive one.
While protective in the short term, this strategy has tradeoffs:
Movements can become less adaptable
Energy cost can increases
Balance corrections can become less automatic
Proprioceptive Changes
Back pain also alters how accurately the body senses position and movement. (16) The proprioceptive system relies on receptors in muscles and joints that continuously inform the brain about body position, allowing you to know where your limbs are even with your eyes closed. Individuals with chronic low back pain often have reduced accuracy detecting trunk position and motion.
In practical terms, the brain receives noisier information about where the spine is in space, like a phone call cutting in and out. To compensate, the nervous system often increases stiffness or slows movement, strategies that may feel safer but reduce coordination efficiency.
Postural Strategy Changes
With both motor control and proprioception affected, postural strategies often change as well.
Common patterns include:
Protective movement patterns
Reduced trunk rotation
Slower transitions between positions
Increased trunk stiffness during standing or walking
Studies examining postural sway show individuals with chronic back pain often rely on larger or more rigid corrections instead of smaller, more finely tuned adjustments. (17, 18) While this may temporarily reduce perceived threat, it makes adapting to unexpected disturbances (slips, uneven ground, or sudden movements) more difficult.
Research in a Nutshell
Pain alters nervous system control of movement, often before measurable strength declines.
Over time, these changes in coordination and movement can contribute to:
Inefficient movement patterns
Reduced physical activity
Gradual strength decline
Decreased balance capacity
Increased stress on the spine
This may create a reinforcing cycle; protective movement changes may unintentionally contribute to ongoing discomfort. To understand why, we need to view the spine not just as a structure that moves, but as a sensory organ that informs movement.
The Spine as an Underappreciated Sensory Powerhouse

Most people think of the spine mechanically, a stack of bones and discs designed to support the body and allow bending and twisting. Neurologically, however, the spine serves another equally important function: it is a major source of sensory information for the nervous system.
A High Density of Proprioception
The deep muscles surrounding the spine, particularly the small stabilizing muscles between each vertebra, contain specialized sensory receptors called muscle spindles, which are responsible for fine control and postural regulation. (19, 20)
These receptors continuously report (21):
Muscle length
Rate of movement
Joint position
In addition to generating force, these muscles are thought to provide precise positional feedback to the nervous system, functioning like biological motion sensors. (21) This constant stream of information helps the brain answer a critical question:
Where is my body in space right now?
Functional Role of the Spine in Balance
Because of this sensory richness, the spine likely contributes to balance in several ways at once:
Stabilizing movement through coordinated muscle activation
Informing spatial orientation through proprioceptive feedback
Coordinating balance corrections between the upper and lower body
Located near the body’s center of mass, the trunk is ideally positioned to detect subtle shifts in alignment. Small spinal adjustments can therefore help influence whole-body balance quickly and efficiently.
When sensory feedback from the spine is clear and reliable, balance corrections tend to remain smooth and automatic. When pain alters or interferes with this feedback, the nervous system often compensates by increasing stiffness, reducing movement variability, or relying more heavily on vision, patterns commonly observed in people with back pain. (22, 23)
A Shift in Perspective For Your Back
The back doesn’t just move you, it helps tell your brain where you are in space so movement can occur efficiently.
Seen this way, improving back health may involve more than strengthening muscles or increasing flexibility. It may also require restoring the quality of sensory information and coordination between the spine and the nervous system.
From this perspective, it becomes easier to understand why balance training, even when it doesn’t directly target the painful area, can sometimes produce meaningful improvements in back pain.
The Back Pain ↔ Balance Loop
At this point, we can connect the pieces of back pain and balance. Back pain affects, at least in part, how the nervous system controls movement. Balance depends on accurate information being processed by the nervous system to allow precise control of movement. So rather than asking whether back pain or balance problems come first, a better question is:
What if they reinforce each other?
This is what I’ve come to think of as the Back Pain ↔ Balance Loop, a model that helps explain how these factors may interact.
Direction One: Back Pain → Balance Problems
When pain appears, the nervous system immediately begins protecting the body. These protective adaptations are helpful in the short term but often influence balance in unintended ways.
Research shows several consistent changes:
Altered Proprioception:
Pain can reduce the accuracy of spinal position sense. (16) When sensory input becomes less reliable, the brain has a harder time predicting and coordinating movement. Balance corrections become slower and less precise.
Protective Stiffness:
People with back pain commonly increase trunk muscle co-contraction, essentially bracing the spine. (24, 25) While this may feel stabilizing, excessive stiffness reduces the body’s ability to make small, efficient balance adjustments. Instead of fluid corrections, movement becomes rigid.
Slower Automatic Reactions:
Delayed anticipatory postural adjustments mean the body reacts after movement begins rather than preparing in advance. (26) This delay may be subtle, but balance is largely a game of milliseconds.
Reduced Confidence in Movement:
Pain also changes perception. Individuals often become less willing to move freely, even subconsciously.
Smaller movement exploration
Slower reactions
Increased reliance on cautious strategies.
Importantly, this isn’t psychological weakness, it’s a normal protective output of the nervous system.
Direction Two: Poor Balance → Increased Back Stress
But the relationship doesn’t stop there, it can also feed back into itself. When balance becomes less efficient, the spine itself may experience greater mechanical demands and altered neuromuscular control.
Potential issues from worsening balance:
Inefficient Movement Patterns:
Poor balance may lead to larger or less coordinated corrections to maintain stability. Instead of distributing forces smoothly across the body, movements may become more segmented or abrupt, potentially placing greater demand on the trunk. (22)
Increased Compensatory Muscle Activity:
When coordination decreases, muscles may compensate by working harder or longer than necessary. Research shows increased co-contraction patterns in individuals with instability or pain, which can elevate fatigue and perceived effort during everyday tasks. (11, 24)
Higher Spinal Loading Variability:
Interestingly, research suggests that both too little variability (rigidity) and too much uncontrolled variability (complete lack of stability) may increase tissue stress and reduce movement efficiency. (27) Healthy movement contains controlled variability, small adjustments that distribute load efficiently. Poor balance may disrupt this distribution, potentially increasing localized strain as the body works to maintain stability.
Greater Injury Risk:
When balance responses are slower or less adaptable, unexpected perturbations (a slip, misstep, or sudden reach) are harder to manage. The spine may then be at greater risk of secondary strain or overload, either during a fall or as muscles work harder to maintain balance.
The Cycle
Put together, the process often looks like this:
Back pain → cautious movement → poorer balance → inefficient movement → increased demands on spine → more pain.
What begins as short-term protection can gradually become a persistent movement pattern that reinforces pain.
Infographic Concept: The Back Pain–Balance Loop
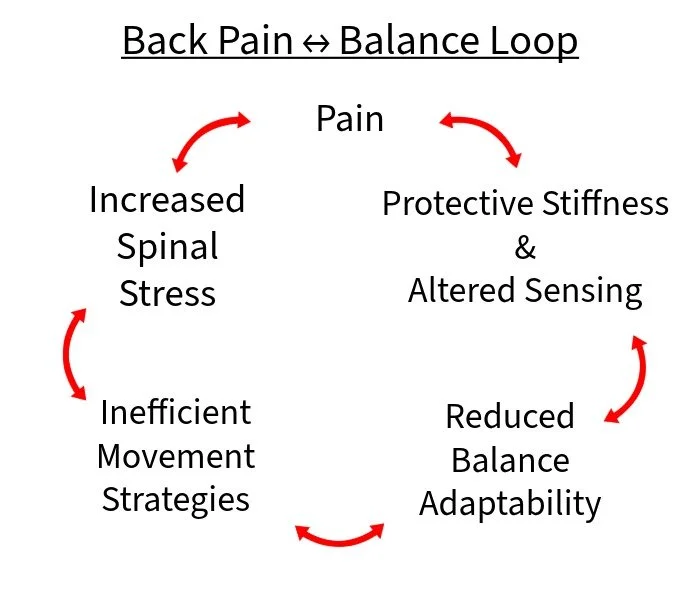
This visual framework helps explain why treating only strength, flexibility, or specific structures sometimes falls short.
The system itself has adapted and needs to relearn coordination. This leads to another interesting question:
Why does balance training, something that doesn’t directly target spinal tissues, often help people with back pain?
Why Balance Training May Reduce Back Pain

When I worked with back pain patients early in my career, balance exercises often improved symptoms even when they didn’t look like traditional “back rehab.” At the time, I wasn’t entirely sure why, but I did know enough to see that it was just as successful (and personally, sometimes more successful) as the typical approaches to rehab with far more enjoyment for my patients.
Modern motor control and pain science now offer several plausible explanations. Balance training may work, in part, not because it strengthens the back directly, but because it changes how the nervous system recognizes and interacts with movement.
Mechanism 1: May Restore Movement Variability
Balance tasks introduce small, safe amounts of unpredictability.
Standing on one leg, reaching, or reacting to instability, forces the nervous system to continuously adjust without being in danger. This reintroduces movement variability, commonly associated with healthy brain motor control. (28)
Research increasingly suggests that persistent pain is associated with overly rigid movement patterns. (11) Balance challenges gently encourage flexibility in coordination again. This can be especially true with more dynamic balance challenges beyond simply standing on one foot.
The body relearns adaptability and slowly allows increased movement.
Mechanism 2: May Improve Sensorimotor Control
Balance exercises demand accurate sensory processing from the body to the brain.
They help:
Recalibrate body awareness, or improve the mind-body connection
Refine joint position sense, your ability to understand where you are in space without looking
Improve integration between sensory input and muscle output
In other words, the nervous system gets better information and makes better decisions about movement.
This aligns with studies showing improvements in proprioception and postural control following sensorimotor training in people with chronic low back pain. (24, 29, 30)
Mechanism 3: May Reduce Threat and Fear
Pain is strongly influenced by perceived threat. (10) Balance training provides graded exposure to instability, small challenges that are manageable and safe while not actually causing any physical injury.
Each successful repetition sends an important signal to the brain: Movement is possible. Movement is safe.
Over time, confidence grows, and protective guarding may decrease. This mechanism is well supported within modern pain neuroscience and exposure-based rehabilitation models. (31)
Mechanism 4: May Activate Low-Load Stabilizers
Unlike isolated strengthening exercises, balance tasks require automatic, coordinated trunk muscle activation. (14) Instead of consciously bracing specific muscles, the body reflexively stabilizes the needed areas to remain upright.
This tends to produce:
coordinated activation,
lower overall muscle tension,
and less guarding behavior.
Research suggests these automatic activation patterns may more closely resemble how stabilization occurs during real-life movement, and specific exercises may not be needed. (32)
Mechanism 5: May Reintegrate Whole-Body Movement
Maybe most importantly, balance training “reconnects” the spine to the rest of the body. The back doesn’t function in isolation, it works within a coordinated system involving hips, legs, vision, somatosensory, and vestibular input. (33)
Balance tasks may help restore this integration. Movement becomes something the whole body shares again, rather than something the spine must manage in isolation during pain.
Signs Your Back Pain May Be Affecting Your Balance

Not everyone with back pain has balance problems. And not every balance issue comes from the back. Humans are amazingly complicated, multiple unrelated problems can exist at the same time.
But there are some common patterns that suggest your back pain may also be influencing how your body maintains stability. Think of these less as diagnoses and more as clues to what may be occurring in your body.
Feeling Unsteady During Standing or Walking
Many people describe a subtle sense of instability rather than obvious imbalance.
You may notice:
Feeling less steady when standing still
Needing to shift position frequently
Feeling slightly unsure when walking in crowded or busy environments.
Individuals with chronic low back pain often demonstrate increased postural sway, small unconscious movements used to maintain balance, even when they don’t consciously feel unstable. (34)
Frequent Near-Trips or Loss of Footing
You may not be falling, but you might notice a need to catch yourself more often.
Examples include:
Misjudging steps
Catching your toe unexpectedly
Needing quick corrective movements to recover balance
These moments often reflect delayed or less efficient automatic balance responses rather than weakness.
Difficulty Standing on One Leg (Especially if Pain Increases)
Single-leg stance is a surprisingly demanding whole-body coordination task.
If standing on one leg feels unusually difficult, or provokes back discomfort, it may indicate altered trunk control or protective muscle activation.
Studies have shown people with low back pain often adopt different trunk stabilization strategies during single-leg tasks, suggesting the nervous system is working harder to maintain control and avoid pain. (35)
Increased Stiffness When Moving Quickly
Many people with back pain feel relatively comfortable moving slowly, but feel stiff or guarded during faster movements.
Quick movements require anticipatory postural adjustments, the brain preparing the body before motion occurs. When these adjustments are delayed or altered, movement can feel tense or unpredictable. The brain may then instead attempt a shotgun approach style of protection by stiffening everything during faster movement. In fact, people with low back pain may actually have a momentary instance of “freezing” before these movements in preparation of the faster movements. (36)
Worsening Discomfort During Transitions
Transitions, moving from one position or place to another, challenge balance more than steady positions.
You might notice discomfort during:
Sitting to standing
Turning
Bending and returning upright
Getting in or out of a car
These movements require coordinated timing between sensory input and muscle activation, precisely the processes often affected by pain.
Avoidance of Uneven Surfaces
Gravel paths, grass, hiking trails, or busy environments may start to feel more of a challenge, leading to avoidance. This avoidance is understandable as uneven terrain can increase sensory and motor demands on the body and back alike.
But over time, avoiding ground variability can reduce exposure to the very stimuli that help maintain adaptable balance.
An Important Note and Clarification
These signs are common and changeable, but they are not proof that your back pain is causing balance problems. People can absolutely have separate, unrelated issues.
However, because balance training is generally low-risk and highly adaptable, these signs represent low-hanging fruit, areas worth addressing that may positively influence both stability and comfort.
Sometimes improving how you move changes how you feel, and at vary least can increase your movement confidence early in the rehab process.
What Research Suggests Actually Helps

If back pain and balance may influence each other, the next logical question is:
What interventions improve both?
The encouraging answer from research is that effective approaches tend to focus less on isolated structures and more on improving how the body coordinates movement as a system all at once.
Importantly, this does not mean forgetting about traditional rehabilitation. It means integrating it all together.
Balance and Proprioceptive Training
Sensorimotor and balance training have shown consistent benefits in people with chronic low back pain, including (37, 38):
Improved postural control
Reduced pain intensity
Improved functional movement
These exercises challenge the nervous system to process sensory information more accurately and respond more efficiently.
Examples include:
Single-leg balance
Reaching tasks
Unstable or variable surfaces
Multi-directional stepping patterns
The goal is not instability for its own sake, it is better adaptability.
Motor Control Exercises
Motor control training focuses on improving coordination and timing of trunk muscles rather than maximizing strength. Research supports these approaches particularly for persistent or recurrent low back pain, where altered movement patterns are common. (39)
Exercises often emphasize:
Controlled movement awareness
Smooth transitions
Low-load precision tasks
Rather than forcing movement, they retrain how movement is implemented and performed.
Core Stabilization Programs, Outdated or Still Useful?
This is where nuance matters, and why you won’t get proper back pain advice from a 30 second social media video.
Early rehabilitation models sometimes framed the core as the key to improving back pain. Modern research has moved away from this idea to a degree, although the “cores” role in back pain is still quite present especially with older clinicians.
However, core stabilization is not outdated, it has simply evolved.
Current understanding suggests:
Low-load stabilization exercises can be useful starting points
Especially useful when pain or fear limits movement acutely
It should only be a starting point, should progress toward dynamic, whole-body tasks.
In other words:
Core training works best when it becomes a bridge at the beginning of rehab, not the destination. (40)
Balance training naturally encourages this progression because stabilization happens automatically within movement rather than through conscious bracing, while also working on multiple body systems simultaneously.
Multi-System Rehabilitation Approaches
The strongest evidence increasingly supports integrated programs that combine:
Strength
Mobility
Balance
Movement retraining
No single component appears sufficient alone. When these elements work together, improvements tend to be larger and longer lasting. Strength training is valuable. Mobility work is valuable. Balance training is valuable. The mistake is treating them as competing philosophies.
The human body does not separate movement into categories like we do in textbooks, and rehabilitation likely shouldn’t either. Strength provides capacity. Mobility provides access. Balance provides coordination. Together, they create resilient movement.
Practical Ways to Begin Improving Balance and Back Health

If balance and back pain influence each other, the question becomes:
Where do you start?
The encouraging news is that improving balance does not require complicated equipment or athletic ability. Many effective starting points look surprisingly simple, because the goal is not intensity, but better coordination.
These are not meant to replace individualized rehabilitation, but rather to introduce safe ways to reconnect movement, awareness, and confidence in your own space and time.
Start With Supported Single-Leg Standing
Standing on one leg challenges coordination throughout the entire body, especially the trunk. It’s the classic balance starting point.
Begin by:
Standing near a counter or wall
Lightly touching for support as needed
Lifting one foot just slightly off the ground
Hold for desired time
The goal is not perfect stillness. Small adjustments are normal, they are your nervous system practicing balance corrections. You’ll become more still as your balance improves.
Add Weight Shifts Into Daily Life
Balance improves through repetition, not isolation.
Simple opportunities for practice include:
Gently shifting weight side to side while brushing your teeth
Rocking forward and backward while standing at a counter
Becoming aware of how pressure moves through your feet, ideally working to be even when stationary
These small movements retrain sensory awareness without feeling like exercise. After all the goal is to get back to living your life.
Practice Reaching While Standing
Reaching introduces controlled instability, something the body must learn to manage safely.
Try these moves:
Reaching forward or sideways while standing
Returning slowly to your upright starting position
Keeping movements comfortable and controlled.
This mimics real-life balance demands far better than static exercises alone.
Walk on Varied Surfaces
Whenever safe, expose yourself and walk on slightly different environments:
Grass
Trails
Sand
Uneven sidewalks
Variation teaches adaptability. The nervous system becomes better at responding to change rather than avoiding it because it learns that it can handle the stresses.
Progress Carefully to Eyes-Closed Challenges
Vision contributes heavily to balance. Removing it temporarily increases reliance on proprioception and vestibular input in a process called sensory reweighting.
Simple progressions include:
Standing with eyes closed for a few seconds
Standing in tandem stance with eyes closed
Standing on one leg with eyes closed
Safety always comes first. Use a counter or other external support as needed for safety.
General Guidelines
Across all balance and rehab work:
Stay within pain-free or tolerable ranges. Ideally less than 3/10 pain
Progress gradually
Prioritize safety and confidence over difficulty
Improvement comes from consistent exposure, not pushing limits.
(A deeper exercise framework will be covered in a future companion article.)
Why My Patients Often Enjoyed Balance Training More

When I first began integrating balance work into sessions with back pain patients early in my career, something unexpected happened. Patients didn’t just improve, they started looking forward to therapy. At the time, I couldn’t fully explain why. I just knew I was trying to make rehab more engaging. Looking back, both research and experience now point to a clearer answer.
Traditional rehabilitation often centers on sets, repetitions, and isolated exercises. Useful, but sometimes mechanical and uninspiring from a patient perspective. Balance training feels different because it is task-based. Instead of thinking about muscles, patients focus on goals like stay steady, reach safely, don’t lose balance, and throw the ball accurately. The brain naturally engages with challenges more than repetition.
Balance work also introduces something rarely discussed in rehab, play.
Small challenges create curiosity and problem-solving, while immediate feedback lets the body feel when movement becomes smoother or more controlled. Each success becomes evidence that movement is safe again. Confidence builds through experience, not reassurance alone. And when people enjoy what they’re doing, they stick with it.
One of my favorite clinic exercises became a kind of game. We would stand about 10 feet apart, each on one leg, throwing a 3–5 lb ball back and forth. The rule was simple, the round ended when you made me put my second foot down.
Sometimes it was over quickly. Sometimes it turned into a long, competitive battle.
What most patients didn’t know was that balancing (walking rails, beams, jumping between small surfaces) was already a big part of my own training. Beating me became a goal. And when it finally happened, it was a highlight of their rehab.
Over time, I started creating new balance challenges each week, not just to progress difficulty, but to keep sessions engaging. Because sometimes the most effective exercise isn’t the most precise one. It’s the one people actually want to do.
Final Thoughts: Balancing Back Pain

Back pain is often treated as a problem of structure like weak muscles, tight tissues, or worn joints. But many cases may be related to problems of coordination and overuse. Pain changes how the nervous system controls movement, altering how we sense position, respond to instability, and interact with gravity itself. Over time, movement becomes cautious and rigid, not necessarily because the body is incapable, but because it is trying to protect itself.
Balance may sit at the center of this process in some instances.
It is the ongoing conversation between sensation and movement, the brain constantly predicting and correcting to keep us upright. When balance improves, the body often regains adaptability, confidence, and efficiency. This may be why balance training can reduce back pain, not by directly “fixing” the spine, but by teaching the nervous system that movement is safe again.
While these ideas are still being explored in research, viewing back pain through the lens of balance may help connect several findings that are often studied in isolation.
What’s Your Fall Risk Score?
Most people don’t notice their balance declining until something goes wrong.
This 10-minute self-assessment will show you:
• How stable your balance really is
• Where you're most at risk (strength, coordination, or falling ability)
• What to focus on first
No equipment. No guesswork. Just clear answers.
References
Zatsiorsky VM, Duarte M. Rambling and trembling in quiet standing. Motor Control. 2000;4(2):185-200. doi:10.1123/mcj.4.2.185
Kroker P. The problem of remaining upright. BMJ. 1999;319(7220):1300. doi:10.1136/bmj.319.7220.1300
Massion J. Postural control system. Current Opinion in Neurobiology. 1994;4(6):877-887. doi:10.1016/0959-4388(94)90137-6
Winter D. Human balance and posture control during standing and walking. Gait & Posture. 1995;3(4):193-214. doi:10.1016/0966-6362(96)82849-9
Goldring MB. The link between structural damage and pain in a genetic model of osteoarthritis and intervertebral disc degeneration: A joint misadventure. Arthritis & Rheumatism. 2009;60(9):2550-2552. doi:10.1002/art.24771
Maus T. Imaging the back pain patient. Physical Medicine and Rehabilitation Clinics of North America. 2010;21(4):725-766. doi:10.1016/j.pmr.2010.07.004
Hutchins TA, Peckham M, Shah LM, et al. ACR Appropriateness Criteria® Low Back Pain: 2021 update. Journal of the American College of Radiology. 2021;18(11):S361-S379. doi:10.1016/j.jacr.2021.08.002
Regev GJ, Treister R, Brill S, et al. Low back pain patients’ perceptions regarding their own radiology reports: Pre-Intervention survey. Journal of Pain Research. 2023;Volume 16:933-941. doi:10.2147/jpr.s396844
Hall AM, Aubrey-Bassler K, Thorne B, Maher CG. Do not routinely offer imaging for uncomplicated low back pain. BMJ. 2021;372:n291. doi:10.1136/bmj.n291
Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976-1982. doi:10.1097/j.pain.0000000000001939
Hodges PW, Tucker K. Moving differently in pain: A new theory to explain the adaptation to pain. Pain. 2010;152(3):S90-S98. doi:10.1016/j.pain.2010.10.020
O’Sullivan P. Diagnosis and classification of chronic low back pain disorders: Maladaptive movement and motor control impairments as underlying mechanism. Manual Therapy. 2005;10(4):242-255. doi:10.1016/j.math.2005.07.001
Hodges PW, Richardson CA. Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Archives of Physical Medicine and Rehabilitation. 1999;80(9):1005-1012. doi:10.1016/s0003-9993(99)90052-7
Hodges PW, Richardson CA. Contraction of the abdominal muscles associated with movement of the lower limb. Physical Therapy. 1997;77(2):132-142. doi:10.1093/ptj/77.2.132
Thomas JS, France CR, Sha D, Wiele NV, Moenter S, Swank K. The effect of chronic low back pain on trunk muscle activations in target reaching movements with various loads. Spine. 2007;32(26):E801-E808. doi:10.1097/brs.0b013e31815d0003
Yang QH, Wang XQ. Lumbar joint position sense measurement of patients with low back pain. EFORT Open Reviews. 2023;8(8):639-650. doi:10.1530/eor-23-0077
Park J, Nguyen VQ, Ho RLM, Coombes SA. The effect of chronic low back pain on postural control during quiet standing: A meta-analysis. Scientific Reports. 2023;13(1):7928. doi:10.1038/s41598-023-34692-w
Xiao W, Yang H, Wang Z, et al. Postural Control of Patients with Low Back Pain Under Dual-Task Conditions. Journal of Pain Research. 2023;Volume 16:71-82. doi:10.2147/jpr.s392868
Ge W, Pickar JG. Time course for the development of muscle history in lumbar paraspinal muscle spindles arising from changes in vertebral position. The Spine Journal. 2007;8(2):320-328. doi:10.1016/j.spinee.2007.05.009
Liu JX, Thornell LE, Pedrosa-Domellöf F. Muscle spindles in the deep muscles of the human neck: a morphological and immunocytochemical study. Journal of Histochemistry & Cytochemistry. 2003;51(2):175-186. doi:10.1177/002215540305100206
Kröger S, Watkins B. Muscle spindle function in healthy and diseased muscle. Skeletal Muscle. 2021;11(1):3. doi:10.1186/s13395-020-00258-x
Van Dieën JH, Reeves NP, Kawchuk G, Van Dillen LR, Hodges PW. Motor control changes in low back pain: divergence in presentations and mechanisms. Journal of Orthopaedic and Sports Physical Therapy. 2018;49(6):370-379. doi:10.2519/jospt.2019.7917
Alrwaily M, Sparto PJ, Whitney SL. Perception of verticality is altered in people with severe chronic low back pain compared to healthy controls: A cross-sectional study. Musculoskeletal Science and Practice. 2019;45:102074. doi:10.1016/j.msksp.2019.102074
Du W, Li H, Omisore OM, Wang L, Chen W, Sun X. Co-contraction characteristics of lumbar muscles in patients with lumbar disc herniation during different types of movement. BioMedical Engineering OnLine. 2018;17(1):8. doi:10.1186/s12938-018-0443-2
Schinkel-Ivy A, Nairn BC, Drake JDM. Investigation of trunk muscle co-contraction and its association with low back pain development during prolonged sitting. Journal of Electromyography and Kinesiology. 2013;23(4):778-786. doi:10.1016/j.jelekin.2013.02.001
Knox MF, Chipchase LS, Schabrun SM, Romero RJ, Marshall PWM. Anticipatory and compensatory postural adjustments in people with low back pain: a systematic review and meta-analysis. The Spine Journal. 2018;18(10):1934-1949. doi:10.1016/j.spinee.2018.06.008
Stergiou N, Decker LM. Human movement variability, nonlinear dynamics, and pathology: Is there a connection? Human Movement Science. 2011;30(5):869-888. doi:10.1016/j.humov.2011.06.002
Stergiou N, Harbourne RT, Cavanaugh JT. Optimal movement variability. Journal of Neurologic Physical Therapy. 2006;30(3):120-129. doi:10.1097/01.npt.0000281949.48193.d9
Rüger A, Laudner K, Delank KS, Schwesig R, Steinmetz A. Effects of Different Forms of Sensorimotor Training on Postural Control and Functional Status in Patients with Chronic Low Back Pain. Journal of Personalized Medicine. 2023;13(4):634. doi:10.3390/jpm13040634
Hwang JA, Bae SH, Kim GD, Kim KY. The effects of sensorimotor training on anticipatory postural adjustment of the trunk in chronic low back pain patients. Journal of Physical Therapy Science. 2013;25(9):1189-1192. doi:10.1589/jpts.25.1189
Woods MP, Asmundson GJG. Evaluating the efficacy of graded in vivo exposure for the treatment of fear in patients with chronic back pain: A randomized controlled clinical trial. Pain. 2007;136(3):271-280. doi:10.1016/j.pain.2007.06.037
Unsgaard-Tøndel M, Fladmark AM, Salvesen Ø, Vasseljen O. Motor control exercises, sling exercises, and general exercises for patients with chronic low back pain: a randomized controlled trial with 1-Year follow-up. Physical Therapy. 2010;90(10):1426-1440. doi:10.2522/ptj.20090421
Sueki DG, Cleland JA, Wainner RS. A regional interdependence model of musculoskeletal dysfunction: research, mechanisms, and clinical implications. Journal of Manual & Manipulative Therapy. 2013;21(2):90-102. doi:10.1179/2042618612y.0000000027
Alshahrani A, Reddy RS, Ravi SK. Chronic low back pain and postural instability: interaction effects of pain severity, age, BMI, and disability. Frontiers in Public Health. 2025;13:1497079. doi:10.3389/fpubh.2025.1497079
Jones SL, Henry SM, Raasch CC, Hitt JR, Bunn JY. Individuals with non-specific low back pain use a trunk stiffening strategy to maintain upright posture. Journal of Electromyography and Kinesiology. 2011;22(1):13-20. doi:10.1016/j.jelekin.2011.10.006
Bourigua I, Simoneau EM, Leteneur S, Gillet C, Ido G, Barbier F. Chronic low back pain sufferers exhibit freezing-like behaviors when asked to move their trunk as fast as possible. The Spine Journal. 2013;14(7):1291-1299. doi:10.1016/j.spinee.2013.11.051
Engel T, Niederer D, Arampatzis A, et al. Sensorimotor stabilization Exercises with and without behavioral treatment in low back pain: Feasibility and effects of a multicenter randomized controlled trial. Archives of Rehabilitation Research and Clinical Translation. 2025;7(1):100430. doi:10.1016/j.arrct.2025.100430
Gatti R, Faccendini S, Tettamanti A, Barbero M, Balestri A, Calori G. Efficacy of trunk balance exercises for individuals with chronic low back pain: a randomized clinical trial. Journal of Orthopaedic and Sports Physical Therapy. 2011;41(8):542-552. doi:10.2519/jospt.2011.3413
Xu HR, Zhang YH, Zheng YL. The effect and mechanism of motor control exercise on low back pain: a narrative review. EFORT Open Reviews. 2023;8(7):581-591. doi:10.1530/eor-23-0057
Coulombe BJ, Games KE, Neil ER, Eberman LE. Core stability exercise versus general exercise for chronic low back pain. Journal of Athletic Training. 2016;52(1):71-72. doi:10.4085/1062-6050-51.11.16